How We Help At-Risk Organizations
Physicians and organizations with at-risk patient populations benefit in a variety of ways from utilizing hospice care for appropriate patients at the end of life.
Members of Medicare Advantage plans are eligible for the Medicare Hospice Benefit.
What Hospice Offers
Hospice patients receive comprehensive, coordinated care, including nursing, home health, pharmaceutical and durable medical equipment. Studies show that patients receiving hospice care often live longer than those not receiving hospice care and that hospice is a more cost-effective way to care for patients near the end of life.
Reduction in Hospital Deaths, ICU Admissions and 30-Day Readmissions
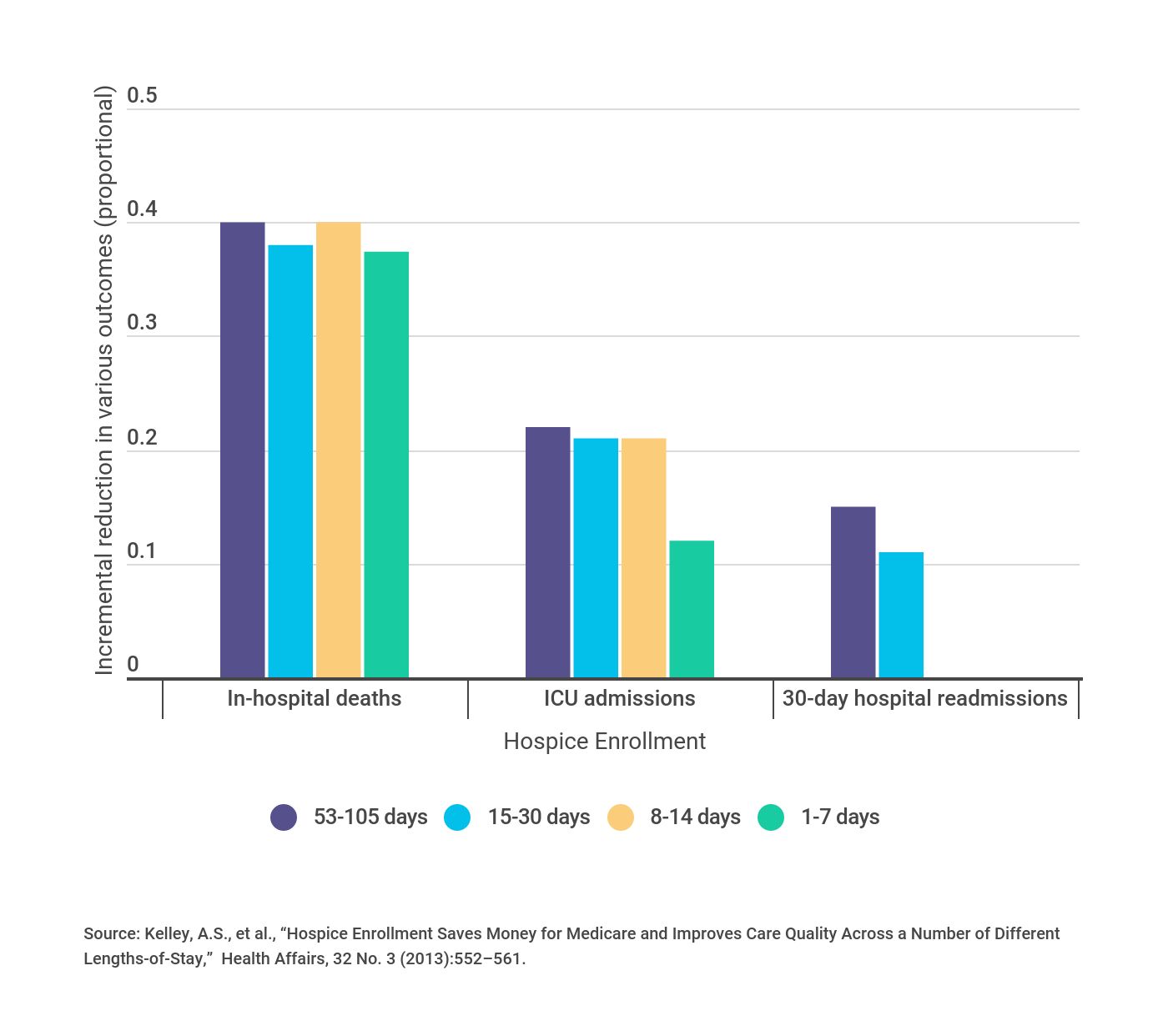
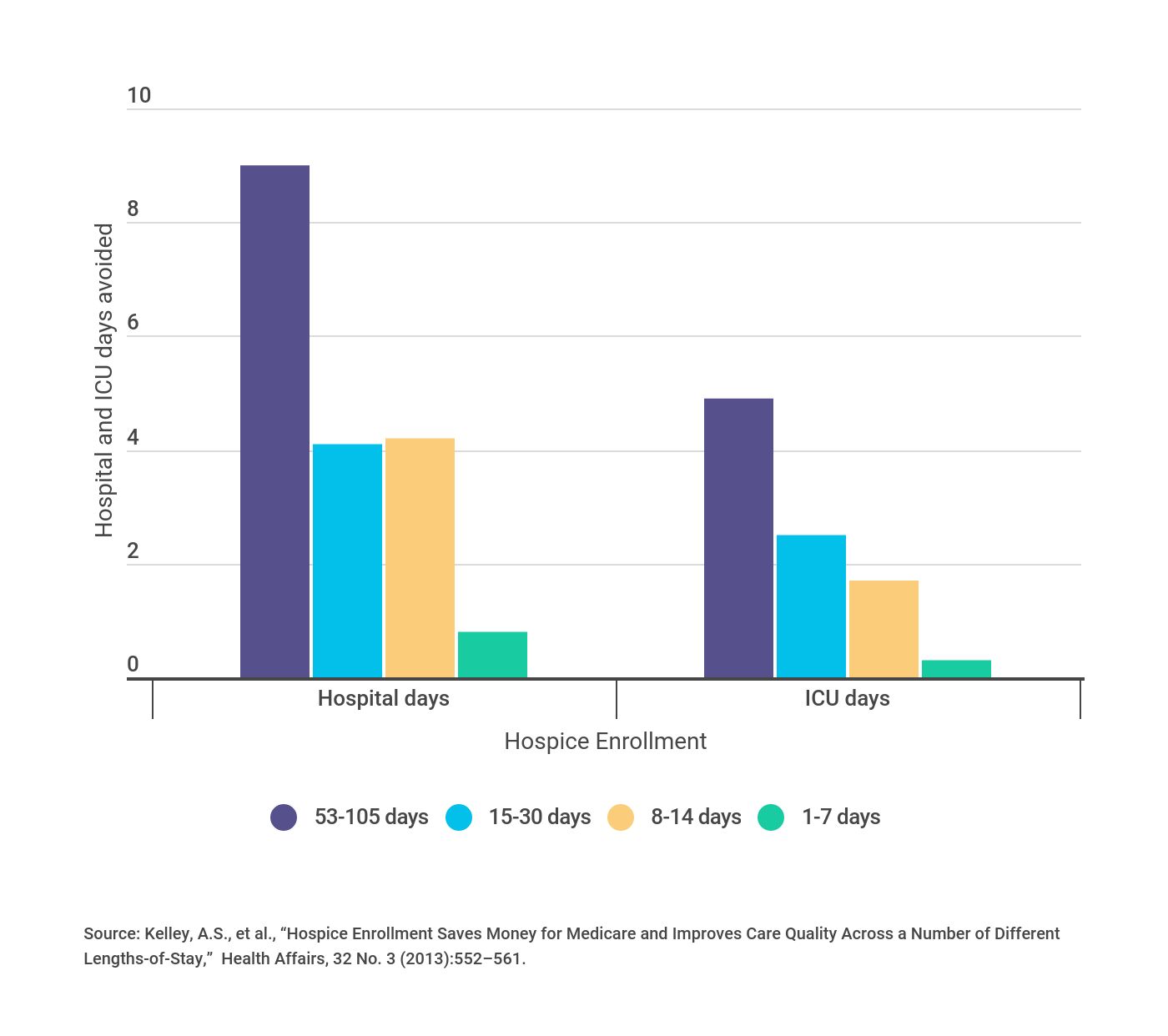
Using fewer hospital services reduces costs and improves both quality of care and the patient’s quality of life. Hospice enrollment resulted in significant reductions in hospital and ICU days. In fact, as the period of hospice enrollment lengthens, the benefits increase.
Reduction in Hospital Days and ICU Days
Reimbursement Considerations for At-Risk Patients on Hospice
During the time the election is in effect, the HMO or CMP may bill Medicare Part A on a fee-for-service basis (subject to the usual Medicare rules for payment) for only the following covered Medicare services:
- Services of the enrollee’s attending physician if the physician is an employee or contractor of the HMO or CMP and is not employed by or under contract to the hospice provider.
- Services not related to the treatment of the terminal condition for which hospice care was elected or to a condition related to the terminal condition.
- Services furnished after the revocation or expiration of the patient’s hospice election until the full monthly capitation payments begin again.
The physician may bill Medicare Part B as FFS for services related and/or not related to the terminal illness. Any PCP employed by hospice would send a physician-services bill to the hospice.
Monthly capitation payments are reduced on the first day of the month after the beneficiary has signed the hospice election form titled “New Enrollee.” Payments begin on the first day of the month after the beneficiary has revoked or expired their hospice election.
Code Modifications for Hospice
Below are the code modifiers used instead of an attestation statement when billing Medicare for hospice care oversight:
- GV—hospice-related diagnosis; attending physician is not employed or paid under arrangement by the patient’s hospice provider
- GW–non-hospice-related diagnosis; service not related to the hospice patient’s terminal diagnosis
- Q5—use in conjunction with GV or GW modifier when another physician in the same practice is covering for the patient’s attending physician
- Q6—use in conjunction with GV or GW modifier when another physician in a different practice or a locum tenens physician is covering for the patient’s attending physician
Speak with your VITAS representative about ways to educate your patients about their hospice alternatives near the end of life. As the nation’s leading hospice provider, VITAS has the experience and resources to assist.